Final exam short case
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis"
Cheif complaints:
70 Year old female patient presented to OPD with the cheif complaints of sob since 5 days and also complaints of vomitings since morning, loose stool 2-3 episodes,
HISTORY OF PRESENT ILLNESS :
Patient apparently asymptomatic 3 years ago
Patient went to regular check up diagnosed with Hypertension and on Regular medication .
Patient was able to do her work previously , from 4 days back she was unable to do her work with grade 2 sob which was progressed to grade 4 sob
Vomitings Since today 3-4 episodes ,food particles as a content
Complaints of Loose stools, 2- 3 episodes
C/0 lump over left back ,tenderness present and no local rise of temperature,
Complaints of decreased urine output since 10 days
No complaints of burning micturition
No complaints of fever ,cough ,cold
No pain abdomen
PAST HISTORY:
History of Hypertension and on regular medication since 2 years . No history Dm,Asthma, epilepsy ,TB,CAD
PERSONAL HISTORY:
Diet: mixed
Appetite : normal
Bowel and bladder : loose stool
No addictions
No known allergies,
FAMILY HISTORY - Not significant!
GENERAL EXAMINATION:
Pallor - present
Icterus - absent
Cyanosis - absent
Clubbing- absent
Lymphedenopathy - absent
Edema - absent
VITALS :
Temp - afebrile
Bp -90 /60 mmhg
Spo2- 95% at room air
RR - 32cpm.
SYSTEMIC EXAMINATION :
Cvs - S1S2 heard,no murmurs heard
Wheeze - absent
Dysponea - present
Position of trachea - central
Breath sounds - normal vesicular sound heard
Adventitous sounds - basal crepts heard
P/A :
obese abdomen ,soft and non tender
CNS :
NAD

Investigation-
ECG 
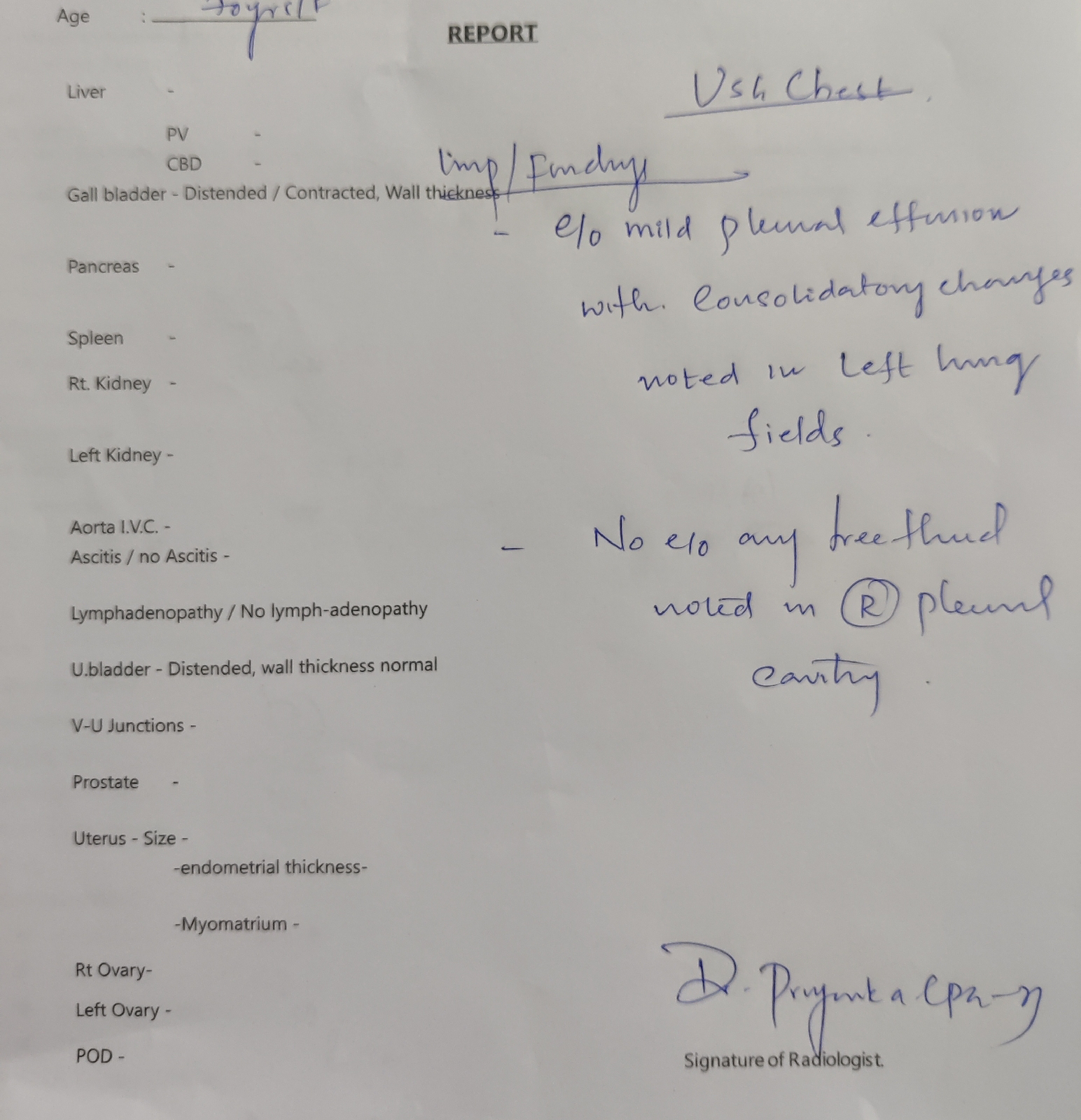

USG abdomen 

Chest X Ray

Treatment -
Treatment -
1.INJ MEROPENEM 500 MG IV BD
2.INJ CLINDAMYCIN 600 MG IV TID
3.INJ HYDROCOT 100 MG IV BD
4.NEBULISATION WITH DUOLIN AND BUDECORT 6HRLY
5.IVF NS @30 ML + OU
6.INJ PAN 40 MG IV OD
7 . INTERMITTENT CPAP 6TH HRLY
8.INJ VANCOMYCIN 1 GM IN 100 ML NS OVER 1 HR OD


Comments
Post a Comment